
FAQ: COVID19 and disability organizations
Many authorities created apps to support in tracking the infection, with self-diagnosing and with practical tips. Unfortunately, we don’t know any accessible Apps.
Denmark
Chatbot that indicates what people with symptoms should do – call a doctor, stay at home or other options. It is not fully accessible but can be used by a screen reader user.
We are very concerned by the situation of persons with disabilities living in institutions. The estimated 1 million persons with disabilities that live segregated in residential institutions are now more vulnerable than ever as they face increased risk of infection by COVID-19, physical and psychological abuse due to isolation, neglect, and abandonment.
Reports show this is already happening in several countries
- Lack of personal protective equipment for persons with disabilities and staff of institutions leads to higher risk of infection- for both staff and residents. The risk is compounded due to the communal life typical of institutions;
- Lack of care and residents left unattended due to staff shortage – staff cannot work as they are infected or under quarantine, or do not work because of fear of becoming infected;
- Forced medication and forced restraint measures under the pretence of preventive measures;
- Forced confinement leading to lack of contact with outside world – family, friends and others.
Denmark
Residential institutions and psychiatric wards in hospitals are considered vital functions to be maintained. The service has been adapted to less physical contact and increased focus on hygiene. Clear guidelines have been adopted (after a period of uncertainty) stating that persons with disabilites in institutions can visit/be visit as long as they comply with current guidelines of social isolation (2 metres apart and maximum gathering of 10 people).
France
In Alsace, the manager of the residential institution “association Marie-Pire” shared with Le Monde discrimination in medical treatment:
A doctor refused to go to the institution to certify a death
On 25 March, the staff called emergency medical services 5 times for 5 different residents. The response they got was to stop calling as the services were over capacity. The medical services didn’t send an ambulance.
The day after the manager had a meeting with the regional health authority. He was told that persons with disabilities would not be received by hospitals. They said they would support the institution with end-of-life care and psychological support for staff.
Greece
Psychiatric units are locking persons in their rooms and depriving them of access to mobile phones and the internet. Contact with family or friends is often prohibited or needs to be done through a single phone, which increases the chance of transmission of COVID-19. Psychiatric units are dealing with staff shortages due to many workers not showing up through fear of being contaminated.
Germany
Residential institutions face a serious lack of personal protective equipment and of funding to support their preventive measures.
We released a statement calling on authorities to act fast on this.
The United Nations Subcommittee on Prevention of Torture has issued a statement.
Italy
70 people became infected in an institution for persons with intellectual disabilities. Managers admitted that residents and staff lacked personal protective equipment;
Poland
52 residents (out of 67) and 8 staff (out of 14) became infected in a residential institution in Poland;
Romania
242 residents and 59 staff became infected in the psychiatric institution Sasca Mică
68 (out of 154) residents and 35 (out of 103) staff are infected with COVID-19 in another psychiatric institution in Costana. Staff was hospitalized but residents were not.
Spain
The press reported several of these cases, including 43 deaths in a retirement home and at least 12 suspected cases in an institution in Granada. There are also reports of support services that are in dire need of masks, gloves and gowns – they are resorting to homemade solutions and are even microwaving equipment in the hope of sterilising them.
Our recommendations
- Make funding and practical solutions available to ensure that persons with disabilities are not negatively affected by the temporary loss of people from their support networks such as personal assistants, family, and specific professional services through illness or indirect impact of COVID-19.
- Designate providers of support services such as care, support workers and personal assistants as ‘key workers’ who should continue to work and be provided with the Personal Protective Equipment (PPE) and instructions on minimising exposure and spread of infection, and be proactively tested for the virus. Workers should be allowed to travel to and from the workplace within organisations or clients’ homes.
- Support agencies providing disability support to develop continuity plans for situations in which the number of available caregivers may be reduced. This includes reducing bureaucratic recruitment barriers while maintaining protection measures such as background checks for caregivers.
Government measures
Some educational systems that remain open for children of key workers (healthcare workers, food shop workers, etc) accept children of parents with disabilities and children with disabilities.
Czechia
Pupils with disabilities should learn at home (with the help of their parents) according to the assignment made electronicaly by their teachers – like any other pupils.The government has adopted measures for the parents of students with disabilities to stay at home with them to help with their education: this is valid for students under 26 years old.
Denmark
Law of March 2020 makes it possible to remove, prioritize or reorganize social services temporarily if needed. However, this does not apply to functions such as residential institutions . There are reports of some municipalities or suppliers that have made general decisions, for example, to close relief programs or discharge children living in a residential institution who have been visiting their family at home. Children with disabilitiess still have the possibility of attending a day care center or school if it benefits the child. The municipalities are obliged to offer emergency care for children with disabilities below the age of 9 years old.
France
Special education units follow distance learning guidance given to all schools. Teachers and education assistants, including for specialized units, continue to work and should provide accessible formats. An exception is made for children with disabilities of healthcare workers: they continued attending school. If persons with disabilities attend day centers, they should remain at home unless their caregivers cannot support them (due to work, or other reasons) – in this case day centers should find a specific solution. If the student with disabilities live in a residential institution, they will stay in the institution and cannot leave (or be visited) until the end of confinement.
Greece
All schools and educational centres are closed. A long-distance educational program was designed for all students, both with and without disabilities. We received reports that doubt that this program will be well implemented by special schools and educational centres for children with disabilities, since they requirs additional educational tools and electronic methods, which, in turn, require more time in order to be able to respond effectively to the unique needs of each student.
Italy
There is extended leave for parents of children until 12. The age limit is waived in case of children with severe disabilities. The leave is recognised alternately to both parents, for a total of fifteen days per month, and is subject to the condition that there is no other parent in the household who is receiving income support due to a suspension or termination of employment or other unemployed or non-worker parent. No other special measures have been taken.
Lithuania
Leave granted to parents that care for persons with disabilities older than 18 years if these persons were in educational programs in vocational schools and/or day centres.
Portugal
Parents of children with disabilities received paid leave and continue receiving the subsidy for assistance (a measure that existed before the pandemic.)
Sweden
Schools and services are not required to close, but shortage of staff is causing problems. Organisations of persons with disabilities are extremely worried with recent demands from local authorities, who requested the central government the ability to prioritise services – there are concerns that this will lead to cuts in the provision of community-based services.
Norway
Customized training is still the teachers responsibility. The national “special education” support system isusually helping schools/pupils in individual cases and with guidance on how to help pupils with learning disabilities such as dyslexia, dyscalculia, developmental language disorders (and others). They have now redeployed resources to staff and enhanced an online chat-service available to both parents directly and teachers.
Spain
The lockdown of the schools excluded educational support for children with disabilities in their first phase of the response (both special schools and extra support). This has been reversed as the country was especially hit by the pandemic and everything closed.
United Kingdom
The Alliance of Inclusive Education provides a complete summary and reaction to the UK’s government decision.
Actions of organisations of persons with disabilities and support services
France
Federation Nationale “Grandir Ensemble” started a platform to support families with children with disabilities.
UNAPEI (the French association of persons with intellectual disabilities) implemented several actions to support students with disabilities and their families: phone helpline, support at home, delivery of educational materials at home and support with education, close follow-up of young children with autism and children with disabilities and behavioural issues, in case of need for respite and in agreement with the Regional Agency for Health, a very partial reopening of an establishment may be considered.
The regional center for autism in the South of France provides support for children and youth with autism through phone calls, special video programmes and daily counseling. The organisation “Association la Bourguette” provides a 24h phone line for support to the families of their students. This support is given by psychologists and teachers from the organisation.
Italy
An association in Milan created an emergency protocol to continue support.
Spain
The ethical guidelines of the Spanish Society of Intensive Care Professionals (Spanish), has an example of what worries:
Page 12, specific recommendations:
“4. Cualquier paciente con deterioro cognitivo, por demencia u otras enfermedades degenerativas, no serían subsidiarios de ventilación mecánica invasiva”
“4. Any patient with cognitive decline, due to dementia and other degenerative disease, will not receive mechanical assisted invasive ventilation.” (roughly translated)
We are very concerned that this excludes a significant population with intellectual disabilities, who have the same chance of survival and the equal right to access healthcare.
Italy
The guidelines of the professionals of anesthesia, resuscitation and intensive therapy (English) are discriminatory:
3. An age limit for admission to the ICU may ultimately need to be set. The underlying principle would be to save limited resources which may become extremely scarce for those who have a much greater probability of survival and life expectancy, in order to maximize the benefits for the largest number of people. In the worst-case scenario of complete saturation of ICU resources, keeping a “first come, first served” criterion would ultimately result in withholding ICU care by limiting ICU admission for any subsequently presenting patient.
4. Together with age, the comorbidities and functional status of any critically ill patient presenting in these exceptional circumstances should carefully be evaluated. A longer and, hence, more “resource consuming” clinical course may be anticipated in frail elderly patients with severe comorbidities, as compared to a relatively shorter, and potentially more benign course in healthy young subjects. In Italy, general criteria for ICU admission were explicitly addressed in a 2003 publication [1] and in a multidisciplinary consensus document released in 2013 for advanced care planning in patients with endstage diseases
United Kingdom
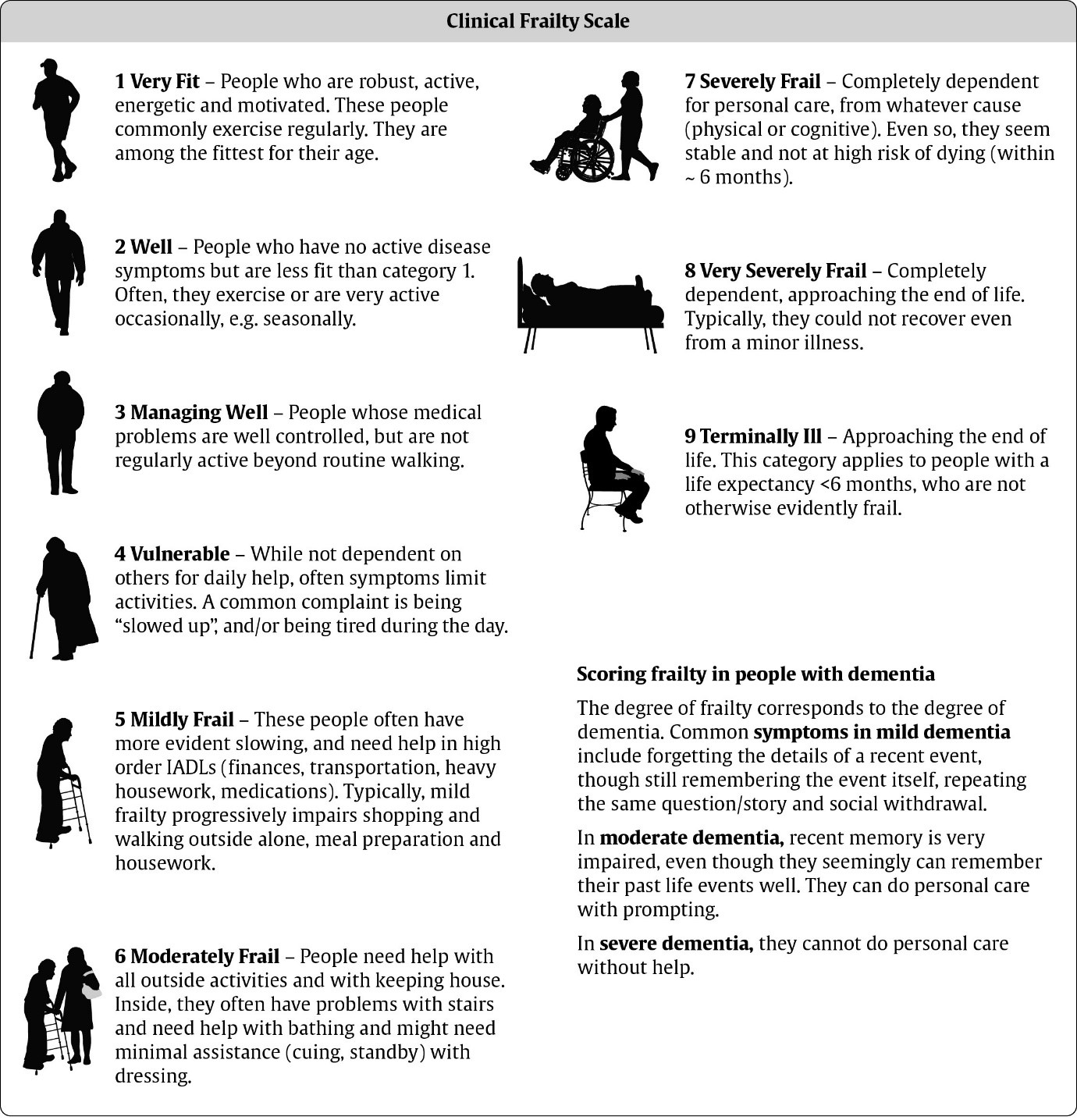
“The guidance from the National Institute for Health and Care Excellence (NICE) says that all adult COVID-19 patients should be assessed for “frailty” when admitted to hospital, and that “comorbidities and underlying health conditions” should be taken into account”.
While this was later updated to exclude certain types of disability (including Cerebral Palsy), it still does not go far enough: It is the use of the CFS “frailty” scoring system that causes most alarm, with the guideline suggesting that those with a score as low as five – those seen as “mildly frail”, who often need help with transportation, heavy housework and medication (nine represents someone who is terminally ill) – might not be considered appropriate for critical care and might be steered towards end-of-life care instead if their condition deteriorated.
{kind=link}
The clarification provided by NICE didn’t go far enough as it still means that certain persons with disabilities (such as learning disabilities) are still in danger of not receiving care:
Maureen Piggot, a member of EDF’s executive committee, said: “I welcome the clarification of the NICE guidelines, but it does not go far enough. The UK needs to follow the UN Convention on the Rights of Disabilities and explicitly ensure that there is no discrimination against persons with disabilities – this includes healthcare guidelines that provide equal access to life-saving support.”
International guidance regarding non-discrimination in prioritisation of patients with COVID-19 (especially in cases of lack of ventilators and bed):
- Our open letter to the World Health Organisation.
- Our recommendations on ethical medical guidelines.
- UN experts: “Everyone has the right to life saving interventions”
- UN Convention on the Rights of Persons with Disabilities (UN CRPD) especially Article 11 – situations of risk and humanitarian emergency
“States Parties shall take, in accordance with their obligations under international law, including international humanitarian law and international human rights law, all necessary measures to ensure the protection and safety of persons with disabilities in situations of risk, including situations of armed conflict, humanitarian emergencies and the occurrence of natural disasters”
- World Medical Association Statement on Medical Ethics in the event of disasters
“In selecting the patients who may be saved, the physician should consider only their medical status and predicted response to the treatment, and should exclude any other consideration based on non-medical criteria.”
- Humanitarian charter of The Sphere
“Any such (humanitarian) assistance must be provided according to the principle of impartiality, which requires that it be provided solely on the basis of need and in proportion to need. This reflects the wider principle of non-discrimination: that no one should be discriminated against on any grounds of status, including age, gender, race, colour, ethnicity, sexual orientation, language, religion, disability, health status, political or other opinion, and national or social origin.”
- The Spanish bioethics committee produced guidance specifically for COVID-19 stating that disability cannot be a factor in ethical medical guidelines.
- The Bioethics Committee of the San Marino Republic produced guidance specifically for COVID-19
“The attribution of priority of treatments to be deliver as well as the victims to be treated cannot fail to take into account the fundamental ethical principles, which materialize in a correct application of triage, trying to optimize the allocation of resources. The only parameter of choice, therefore, is the correct application of triage, respecting every human life, based on the criteria of clinical appropriateness and proportionality of the treatments. Any other selection criteria, such as age, gender, social or ethnic affiliation, disability, is ethically unacceptable, as it would implement a ranking of lives only apparently more or less worthy of being lived, constituting a unacceptable violation of human rights.”
Statements on government measures
- Complaint by the Spanish National Disability Council
- Statement by Italian disability organisations
- Statement by the Belgian National Superior Disability Council
The Council of Europe’s Commissioner for Human Rights states: “It is the foremost duty of all member states to ensure that this does not occur and to reassure people with disabilities that they will not risk discrimination on the basis of disability in accessing health care and that their needs will still be addressed adequately.”